Time is the most complicated factor in medical billing. It can make or break your case. Medical billing takes up a lot of your time and effort, but when you outsource those complex procedures, you can save lots of your time.
However, outsourcing does not mean that you shouldn’t have information regarding the topic when you are completely aware of the procedure/process, time, and rates. It saves a lot of your time on deciding which company to choose and which does not meet your requirements.
Below is the complete guide to medical billing time requirements, rates, and more.
What is CPT Code 99214?
Basically, CPT code 99214 describes an established patient office or outpatient Evaluation and Management (E/M) visit. Providers typically use this code when a patient requires a moderate amount of examination.
Also, there are 3 main rules that doctors have to fulfill when using this code
1. The doctor spends 30 to 39 minutes total on your care that day. This includes talking to you, reading your charts, and writing notes.
2. You have medium-severity health issues. Examples include managing two chronic illness flare-ups or a new illness that affects your whole body.
3. The doctor makes a medium-risk decision. The most common example is writing you a new prescription for a drug.
When they are up to these 3 rules, only then can the provider apply for insurance
2026 Medicare Reimbursement Rates for 99214
The foundation of a healthy revenue cycle is knowing what Medicare will pay when it comes to billing CPT code 99214. For 2026, the Centers for Medicare & Medicaid Services (CMS) finalized reimbursement rates under the CMS-1832-F Physician Fee Schedule Final Rule, and the numbers don’t lie, depending on your practice location. There was a significant increase in office-based providers and a decrease in hospital-based billing.
Beyond the base rate, factors like your geographic location (GPCI adjustments), place of service, and whether you qualify to append the G2211 complexity add-on code matter, and these factors determine how much reimbursement you are going to receive.
The chart below provides a complete breakdown of the national average Medicare rates, RVU components and payer-by-payer comparisons of 2026.




Highlights of the Chart
This chart answers one simple question: “How much money does a doctor get paid for a 99214 visit in 2026?”
The answer is, it depends. Now, let’s go through each part.
1. The Four Big Numbers at the Top
Think of these as the “quick facts” box.
$135.61
Medicare will reimburse the doctor $135.61 if a patient comes to the doctor’s office. This has increased from last year, which is good news for doctors.
$84.50
When the same doctor provides the same care to the same patient, however, at a hospital, Medicare pays $84.50. Why less? It is already separately compensated by the hospital for building and staff usage. Therefore, the doctor receives a smaller percentage.
1.92 (Work RVU)
Consider this as a “difficulty score” for the visit. A 99214 visit has a score of 1.92, which is a moderately complex visit. There was no change in this number in 2026.
$32.35 (Conversion Factor)
Medicare rates this, and then multiplies it by the difficulty score to get the final payment. This year it was a tad lower. Imagine that it were like exchange rates, though your score may be equal, a lower exchange rate would be a smaller amount of money.
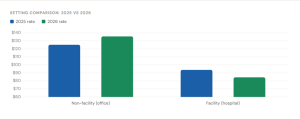
2. The Bar Chart — Office vs Hospital, 2025 vs 2026
This graph only compares the earnings of doctors to those of last year. The blue bar is 2025. The green bar is 2026.
For office visits
The green bar is taller. Medical workers received an increase in pay.
For hospital visits
The green bar is shorter. Doctors got a cut.
The big lesson here is simple: the same visit, the same doctor, the same patient, but the location changes the payment by over $50.
3. The Second Bar Chart — Why Is the Office Rate Higher?
This chart provides an explanation for the $50 difference. There are three components to each payment:
Part 1 — Work (the doctor’s effort)
This is the same in both places, 1.92. Makes sense, because the doctor does the same job whether they are in their clinic or a hospital.
Part 2 — Practice Expense (running costs)
This is where the big difference is. At their own clinic, the doctors pay for rent, electricity, nurses, and equipment themselves. So, Medicare gives them more money to cover that. At a hospital, the hospital pays for all of that, so the doctor gets almost nothing for this part.
Part 3 — Malpractice (insurance cost)
This small number is the same in both places, 0.14. Not a big deal either way.
Add all three parts together, and you get the total score of 4.06 for the office and 2.53 for the hospital. Multiply by $32.35, and you get your final payment.
4. The Table — Who Pays What?
Doctors aren’t only being paid by Medicare. There are other insurance types, too. Let’s compare them:
Medicare — $135.61
This is the standard. Every other payer is compared to this number.
Regular private insurance (like DoctorMGT, Blue Cross, Aetna) — $175 to $225
Private insurance companies typically will cover 20% to 50% more than Medicare. So the same visit that Medicare will pay $135 for, a private insurer could pay $200 for.
Top private insurance contracts — up to $250
A doctor or hospital that has made a great deal with an insurance company will be able to receive as much as $250 for every visit.
Medicaid in low-paying states — around $81 to $95
Government insurance for low-income individuals is called Medicaid. In many states, it pays even less than Medicare, and sometimes only 60 cents out of every dollar Medicare pays.
Medicaid in high-paying states — around $125 to $136
In some states, the Medicaid physicians are compensated significantly more, nearly as much as Medicare.
5. The G2211 Add-On — Bonus Money Most Doctors Miss
This last section is about an extra code called G2211. To put it simply, if you place an order for a burger at $135, imagine that. If your order is more complicated, such as having special dietary requirements, then the restaurant has to charge an additional fee of $16.
This additional fee is G2211.
A visit that involves a doctor treating a patient’s continuing health issues, such as diabetes, blood pressure, and heart disease, is more complicated than the average visit. The doctor can add G2211 to the bill and get back an additional ~$16.57 from Medicare. So instead of $135.61, the doctor collects ~$152.18 for that visit. Most doctors aren’t familiar with this and don’t remember to include it.
This small extra code can cost hundreds of patients thousands of dollars in lost income over the course of an entire year and hundreds of patients.
Time Requirements for CPT Code 99214 in 2026
This is one of the most frequently asked questions providers receive: How can I document a visit as being covered by 99214? The answer is in terms of time and complexity, and in 2026, there will be two reasonable excuses for this code.
Method 1 — Total Time
The doctor should spend 30-39 minutes on the patient’s care on the day of the visit. This is not mean only being in the room face-to-face. It involves looking at previous records prior to visiting the patient, making notes after the patient has left, ordering tests, and liaising with other practitioners. Combining all the above is equivalent to the same day.
Method 2 — Medical Decision-Making (MDM)
A physician could earn 99214 if they can demonstrate that the visit was of moderate complexity, but not always easy to time. To fulfill this standard, two of the following must apply: The patient had more than one health issue, or it was a complicated health issue; The doctor examined a substantial amount of data or test results; The risk level was moderate, including when the doctor prescribed a new medication or ordered a procedure.
Either method works. Most billing specialists recommend documenting both, when possible, as it will strengthen the case in case of an audit.
Medical Decision-Making (MDM) Criteria for 99214
Most 99214 claims are based on MDM. Let’s make this easy to understand!
1. Problem complexity
The patient must have a problem that’s not straightforward. All of these are considered: dealing with two chronic conditions at the same time, having a new illness that gets worse, or handling a condition that doesn’t improve with treatment. A normal check-up of the blood pressure of a stable patient does not.
2. Data reviewed
The physician should verbally demonstrate that they inspected and considered the information. This includes looking at test results, another doctor’s records or interpreting an imaging scan on his or her own. The more data examined and put into practice, the more powerful the MDM argument.
3. Risk level
This is the doctor’s choice. All of the following are considered moderate risk decisions: prescribing a new drug, ordering an IV treatment, or deciding to refer the patient to a specialist. The prescription of more water, rest, and food alone is not.
Getting MDM documentation right is one of the areas where a qualified EMS billing services team adds the most value. They know exactly what language and documentation CMS auditors look for, and they make sure your notes support the code before the claim is ever submitted.
99214 vs 99213 vs 99215: How to Choose the Right Code?
This is a choice that most service providers face on a daily basis. Sub-optimally picking the wrong code is not only an economic loss of money but also the risk of being audited for over-coding or under-coding.
Here is a simple way to think about all three:
- 99213 is used for simple visits. The problem is uncomplicated and low risk. The doctor takes 20-29 minutes and prescribes something that he or she had already done before, such as renewing a prescription or treating a minor infection with a standard antibiotic.
- 99214 is the middle ground. Some degree of complexity, 30 to 39 minutes, and an actual decision with some risk. For good reason, it is the most frequently billed established patient code in the nation.
- 99215 is for the most complex visits. Decision making needs to be complex, time-consuming (40-54 minutes), and decisions could have detrimental consequences for the patient. Imagine patients whose diseases are not controlled or where hospitalization is being considered, who have one or more other uncontrolled diseases.
The truth is that most practices use 99213 and underuse 99215 at the same time, and report the middle code where they should report the high code. The medical billing and coding specialist is trained to detect this sort of pattern. They check your documentation against the actual criteria, and ensure that the code you submit is a clear reflection of the actual level of service, which helps to avoid under and audit risk.
Documentation Requirements to Support a 99214 Claim
Writing more isn’t a problem with Good Documentation; it’s about writing the right things. The following should be clearly indicated on each 99214 note:
1. Chief complaint
So what brought the patient to you today? This must be particular. This is not sufficient: “Follow-up”. The title “Follow-up for poorly controlled Type 2 diabetes with new complaint of foot numbness” reads much better.
2. History of the problem
What changes were seen since the previous inspection? Has the condition improved, worsened, or remained unchanged? Any new symptoms?
3. Examination findings
What did the doctor examine? An examination, to be documented under the 2026 guidelines, does not have to be comprehensive, but it must be medically appropriate to the problem.
4. Assessment and plan
This is the most important part. What did the doctor determine, and why? What do you need to do next? This section should be moderately complex, referring to conditions being addressed, the data being reviewed, and the rationale for the decision that was made.
5. Time attestation (if using the time method)
If the doctor is billing based on total time rather than MDM, the note must include a specific statement like: “Total time spent on this encounter, including pre- and post-visit work, was 35 minutes.”
Missing any of these elements is one of the fastest ways to get a 99214 claim downgraded or denied. Many USA medical billing companies offer documentation audits as part of their services, reviewing your notes before submission to catch gaps that would otherwise result in lost revenue or compliance issues down the line.
Common Billing Mistakes to Avoid with CPT 99214
Even experienced providers make these errors. Knowing them up front saves you from costly corrections later.
1. Using the wrong time range
If the total time is 28 minutes, that is a 99213, not a 99214. Billing 99214 for that visit is upcoding, even if it feels like a moderate visit. Always document the actual time.
2. Vague chief complaints
Notes that say “here for follow-up” without any clinical detail do not support 99214. Auditors need to see that the visit had a real clinical purpose that matches the complexity of the code.
3. Missing the MDM connection
Writing a prescription is not enough the note needs to show that
Telehealth and CPT 99214 in 2026
Good news for providers who offer virtual care 99214 applies to telehealth visits under the 2026 rules, as long as the visit meets the same time or MDM requirements as an in-person visit.
The same 30 to 39 minutes standard applies. The same MDM criteria apply. The documentation requirements are identical. The only real difference is that you need to note in your records that the visit was conducted via audio/video technology and that the patient consented to the telehealth format.
One important update for 2026: CMS introduced new dedicated telehealth CPT codes in the 98000 series for certain visit types. However, for standard established patient evaluation and management visits, 99214 remains the appropriate code. If you are unsure which applies to a specific telehealth encounter, that is the kind of question your billing team should be answering before the claim goes out, not after a denial comes back.
How to Audit Your 99214 Claims for Compliance
Running a self-audit every quarter is one of the smartest things a practice can do. Here is a simple process:
Pull a random sample of 20 to 30 claims billed under 99214 from the past 90 days. For each one, check: Does the note clearly support 30 to 39 minutes of total time OR moderate complexity MDM? Is the chief complaint specific? Does the assessment and plan reflect a real decision? Was G2211 applied where appropriate?
If more than 20% of your sampled claims have documentation gaps, that is a red flag worth addressing immediately, either through provider education or by reviewing your entire billing workflow.
The final piece of advice is this: CPT code 99214 is not complicated in theory, but it is very easy to get wrong in practice at scale. Whether you handle billing in-house or work with an outside partner, the standard should always be the same: every claim submitted should be one you could defend in an audit without hesitation.