A single missed digit on a CPT code can turn a $170 visit into a $57 one, and most primary care practices don’t catch it until the denial lands three weeks later. Since the majority of the claims submitted each day are E/M codes, proper documentation of a primary care CPT isn’t something that is a box to check. It’s the difference between a healthy revenue cycle and a backlog of appeals that eats into staff time and delays cash flow.
This guide breaks down the common and updated CPT codes for primary care practices, how they’re structured, what they actually pay, and where billing teams typically lose money without realizing it.
What Are the Most Common CPT Codes for Primary Care Visits?
The backbone of primary care billing is the Evaluation and Management (E/M) code set. These CPT codes that primary care providers use most often are split into two groups based on whether the patient is new or already established with the practice.
New patient visits (99202–99205) apply the first time a patient walks through the door. This means the visits will be longer because the provider will need to get a full history, baseline vitals, and an initial treatment plan.
Established patient visits (99211–99215) cover everyone already in the system. This is where the majority of the volume is, and where the smallest documentation deficiencies can add up to significant losses in revenue.
|
CPT Code |
Visit Type |
Typical Use Case |
|
99202 |
New patient, straightforward | Healthy adult, first visit |
|
99203 |
New patient, low complexity | New patient, single manageable condition |
|
99204 |
New patient, moderate complexity | New patient with multiple chronic conditions |
|
99211 |
Established, minimal (nurse visit) | Blood pressure check, injection only |
|
99213 |
Established, low complexity | Stable, controlled chronic condition |
|
99214 |
Established, moderate complexity | Medication adjustment, new symptom |
|
99215 |
Established, high complexity | Multiple serious conditions, extensive review |
Of these, 99213 and 99214 typically make up the largest share of daily claims in a primary care practice, since most follow-up visits fall into the “stable but requires clinical judgment” range. Here’s a look at how reimbursement scales across the E/M code range:
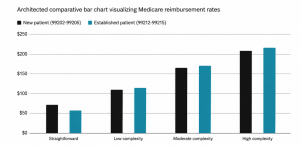
The gap between 99212 and 99215 alone is over $160 per visit, which is exactly why accurate level selection matters so much at scale across a full patient panel.
Why Primary Care CPT Codes Are Harder to Get Right Than They Look?
The variety of codes seen in primary care is greater than in almost any other specialty on a given day. A patient comes in with a sore throat, another patient with an annual physical, another patient with diabetes, and another patient for a vaccine. Every encounter is from a different code family, and there is no clear-cut boundary between families, even for experienced coders.
It’s that diversity that makes primary care CPT codes so much of a hassle to bill downstream. A small percentage of errors can add up to significant lost revenue for a practice that sees 25 or more patients in a day, and payers are diligent about downcoding or denying claims that deviate from the documentation in the record.
The other thing that makes primary care coding so challenging is that, because of the nature of the practice, providers working in primary care are generalists. One visit may cover an ongoing chronic condition, a new acute problem, and a screening for preventive action. But each of those codes can have its own coding implications, and there are several things the person picking the code needs to know: How are multiple services layered on one claim? Each of those codes can have its own coding implications, and there are several things that the person selecting the code needs to know: How are multiple services layered on one claim?
Which CPT Codes Cover Preventive and Wellness Visits?
Preventive care runs on a completely separate code set from problem-focused visits, and mixing the two up is one of the most common billing errors in primary care.
- 99381–99387: Annual physicals for new patients, coded by age group
- 99391–99397: Annual physicals for established patients, also coded by age group
- G0438: Initial Medicare Annual Wellness Visit billed once per patient, ever
- G0439: Subsequent Medicare Annual Wellness Visits billed once per year after that
The down side for billing teams to keep in mind: If, during a preventive visit, a provider treats an actual medical issue (e.g., a patient visits for annual physical and reports increased knee pain), that will require a different E/M code with a modifier 25 attached. That modifier is ignored and the problem-visit code gets lumped into the preventive modifier and is ignored.
This is a challenge even for experienced staff as there is no separation in the visit to the provider, but rather it must be separately coded and documented as two visits. The fix is procedural, not clinical: Educate providers on the boundary of a preventive visit as it turns into a problem-focused visit and ensure that the note clearly differentiates between the two in a way that allows a coder to distinguish between the two.
What CPT Codes Are Used for Chronic Care Management?
Primary care is where chronic disease management actually happens day to day, and there are codes built specifically to reimburse that ongoing work, separate from the office visit itself.
- 99490: First 20 minutes of chronic care management (CCM) per month
- 99439: Each additional 20 minutes of CCM
- 99491: Complex CCM performed directly by the physician
Patients must be known to have two or more chronic conditions with documented consent, and the patient requires a clear time record of the care coordination activities, medication review, care plan changes and specialist calls made, when these services are billed. For the work that these practices are already performing informally on phone calls or portal messages, which never go to the CCM, they are forgoing a recurring monthly revenue stream.
A lot of the administrative lift here is real; someone has to keep track of time and keep up with the activities, and that’s a process that’s easy to formalize, and usually pays off in the first billing cycle for practices that have a large population of diabetic, hypertensive, or COPD patients.
Diagnostic and Procedure Codes Primary Care Practices Bill Daily
Beyond E/M codes, most primary care offices bill a steady stream of smaller, high-frequency codes:
- 36415 — Routine venipuncture
- 93000 — EKG with interpretation
- 81002/81003 — Urinalysis
- 90471/90472 — Immunization administration
- 90686 — Influenza vaccine
- 11200–11201 — Skin tag removal
Each of these is billed on top of the office visit code when performed during the same encounter. And each one gets missed more often than practices realize, especially specimen collection codes. Which frequently go undocumented even though the lab work itself gets billed. Vaccines are one of the more typical gaps: The vaccine product code is two lines and the administration code is two lines, and if either is missing, the entire service is performed but not reimbursed.
Common Billing Mistakes That Cost Primary Care Practices Revenue
A few patterns show up again and again in primary care claims:
Coding by time alone
A 30-minute visit doesn’t automatically justify a high-level code if the medical decision-making was straightforward. Payers check both.
Forgetting modifier 25
This single omission is one of the most common reasons a same-day E/M and procedure claim gets bundled and underpaid.
Under-documenting exam elements
If the note references systems that weren’t actually documented, auditors will downcode the claim on review.
Skipping CCM and TCM billing
Care coordination work that already happens informally often goes completely unbilled.
Using outdated codes
The CPT code set updates every January, and a practice running on last year’s superbill is quietly losing revenue.
Each of these mistakes is individually small, but they compound. A practice that consistently under-codes 99214 visits as 99213, forgets modifier 25 twice a week. And misses CCM billing entirely can be leaving thousands of dollars per provider. Per month, unclaimed without a single denied claim to flag the problem.
Getting the Foundations Right: Internal Medicine Medical Billing and Coding
Practices that treat billing as an afterthought rather than a system are the ones that see the most denials. Solid medical billing and coding starts with documentation that matches the code being billed, not the other way around. This matters just as much for internal medicine medical billing, where patients often carry multiple chronic conditions, and the line between a routine 99213 and a more complex 99214 can hinge on how thoroughly the visit is documented.
Take the 99203 CPT code as an example: it’s meant for a new patient visit with low medical decision-making complexity, but it’s frequently confused with 99202 or 99204 simply because the documentation doesn’t clearly support the level billed. These points are not so much about memorizing a code block range. As creating a documentation habit that will help in whatever code block. That might be submitted, one that can be followed with certainty by a coder and then an auditor with no need to guess.
Ready to Fix Your Primary Care Billing Process?
Primary care CPT coding isn’t simply an office procedure; it is connected to how well a practice is being compensated for the work that is occurring. From E/M levels to the preventive visit codes, chronic care management, and the tiny code for the small procedure. There’s a lot of space for revenue to quietly walk out the door.
The practices that are ahead of this are the ones that conduct regular documentation reviews. Keep up on annual code changes, and identify the modifier errors before claims are submitted. Instead of after a claim is denied weeks later.
When that’s the case and your practice is getting regular denials, downcoded claims. Or is struggling to keep up with annual CPT changes. A billing team well-trained in primary care and internal medicine can fill in those gaps and put money back in your pocket that’s going elsewhere.